
There was a time when the phrase Black-owned felt like a declaration of arrival.
It carried the weight of history, the echoes of exclusion, and the promise of something reclaimed. To build, to own, to operate independently in a system that once denied all three was not merely economic. It was symbolic. It meant that the barriers, however formidable, were not permanent.
I understood that pride. I shared it.
But over time, the meaning of that label began to change. Perhaps more precisely, its application did. What once signaled resilience and entry into the broader marketplace began, in certain cases, to signal something else. Something more fragile. Something more concerning.
To understand that shift, it helps to examine a case that was, in many ways, born from the same spirit that once made Black-owned so powerful: Martin Luther King Jr. Drew Medical Center. King/Drew, as it was often called, did not emerge in a vacuum.
Its origins were rooted in the aftermath of the Watts Riots of 1965, when the lack of adequate medical care in South Los Angeles became impossible to ignore. The hospital was envisioned as a solution, a place that would serve a predominantly Black community with dignity, access, and cultural understanding.
On paper, it represented progress. In spirit, it embodied purpose.
What made Martin Luther King Jr. Drew Medical Center particularly compelling, and ultimately particularly tragic, was how fully it embodied the idea of identity-driven institution building.
The hospital was not merely located in a predominantly Black community. It was intentionally staffed, administered, and culturally oriented to reflect that community. In many respects, it was viewed as a model of what self-determination in critical infrastructure could look like. Black doctors, Black nurses, Black leadership. Representation was not incidental. It was central to the mission.
And for a time, that mission carried enormous symbolic power. But symbolism, however meaningful, proved insufficient as a governing principle.
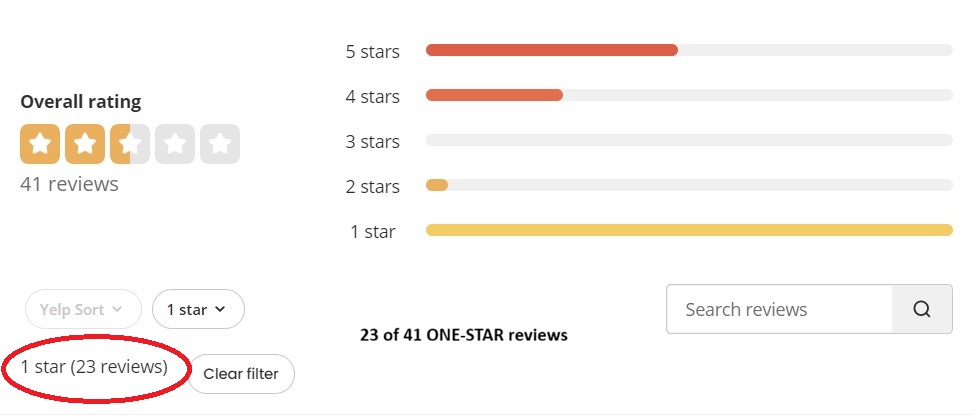
By the early 2000s, a series of federal investigations began to expose deeply troubling patterns within the hospital. Reports from the Centers for Medicare & Medicaid Services documented repeated failures in basic standards of care. Patients were misdiagnosed. Emergency room wait times stretched into dangerous territory. Critical procedures were mishandled.
In one widely cited case, a patient died after languishing in the emergency room for hours with a treatable condition. In another, medical staff failed to follow even the most fundamental protocols, raising questions not just about isolated negligence, but systemic breakdown.
Oversight bodies found that these were not anomalies. They were symptoms.
The hospital’s affiliation with Charles R. Drew University of Medicine and Science, which was intended to create a pipeline of Black medical professionals, became strained under the weight of these failures. Accreditation issues emerged. Training programs were scrutinized. What was meant to be a beacon of advancement began to flicker under regulatory pressure.
Management instability compounded the problem. Leadership turnover was frequent. Accountability mechanisms were weak or inconsistently enforced. Political considerations, according to multiple reviews, often complicated or delayed necessary reforms.
And perhaps most damaging of all, the hospital developed a reputation among regulators as an institution where standards were negotiated rather than upheld.
This is the part of the story that resists easy telling.
Because the failure of King/Drew was not due to a lack of purpose. It was not due to insufficient funding alone. And it was certainly not due to a lack of representation.
It was a failure of execution. The distinction matters.
Because it reveals something deeper than mismanagement. It exposes the limits of a framework that places identity at the center of institutional design without equally centering performance, accountability, and excellence.
By 2007, after years of mounting deficiencies, federal authorities moved to terminate key funding streams. Without them, the hospital could not operate. Its closure marked the end of an experiment that had once been heralded as a milestone in community empowerment.
What remained was not just a shuttered facility, but a cautionary tale.
 Economist Thomas Sowell has long argued that good intentions, particularly when tied to group identity, cannot replace the hard requirements of competence and performance. In Discrimination and Disparities, he emphasizes that disparities in outcomes often reflect differences in skills, incentives, and institutional structures rather than solely the presence of discrimination.
Economist Thomas Sowell has long argued that good intentions, particularly when tied to group identity, cannot replace the hard requirements of competence and performance. In Discrimination and Disparities, he emphasizes that disparities in outcomes often reflect differences in skills, incentives, and institutional structures rather than solely the presence of discrimination.
Applied to King/Drew, the lesson is stark.
A mission rooted in service to a specific community does not exempt an institution from the universal standards that govern its field. In healthcare, those standards are unforgiving, as they should be. Lives depend on them.
Economist Walter E. Williams frequently warned that when institutions are shielded from rigorous competition or sustained by political considerations rather than performance, their quality tends to decline. Incentives matter. Accountability matters.
If an institution is evaluated less on outcomes and more on its symbolic importance, a dangerous imbalance can emerge. Criticism becomes muted. Standards become flexible. And over time, the very people the institution was meant to serve bear the cost.
Justice Clarence Thomas has similarly expressed concern, in both his opinions and his autobiography, My Grandfather’s Son, about the long-term effects of systems that frame Black advancement through exception rather than expectation. His perspective underscores a principle that resonates here: dignity is not preserved by lowering the bar. It is preserved by meeting it.
The story of King/Drew does not invalidate the concept of Black ownership or Black-led institutions. That would be an overreach. But it does challenge the assumption that identity, even when rooted in legitimate historical grievances, can serve as a foundation for sustained success.
It cannot.
Because in the end, every institution, whether a hospital, a business, or a financial enterprise, is judged by the same metric: performance.
This brings us back to the broader cultural use of the term Black-owned.
When the label functions as a marker of excellence earned within the full spectrum of competition, it is not only appropriate, it is admirable. But when it becomes a shield, or worse, a substitute for excellence, it begins to erode the very progress it was meant to signify.
The danger is not always overt. It often appears in small ways: lowered expectations, selective accountability, or the quiet assumption that support should be extended regardless of outcome.
Those patterns, if left unchallenged, accumulate.
And over time, they reshape perception.
Instead of signaling achievement, the label risks signaling qualification. Instead of inviting confidence, it invites scrutiny. Not because of prejudice alone, but because of precedent.
That is the legacy that must be confronted honestly.
The aspiration should not be to abandon identity, but to ensure that it never eclipses performance. The goal is not separation, but integration. Not symbolic success, but substantive success.
Because the marketplace, like medicine, is ultimately indifferent to intention. It responds to results.
And if the next generation of Black entrepreneurs and institutions is to build something enduring, something that commands respect without qualification, then the lesson of King/Drew must be taken seriously.
Not as a condemnation. But as a course correction.
A reminder that the most powerful statement any enterprise can make is not who it serves, or who built it, but how well it fulfills its purpose.
Everything else is secondary.

